



Let us help you find what you’re looking for
What is - Caring for Your Tracheostomy
 On this page, you will learn more about tracheostomy and how you can care for it at home.
On this page, you will learn more about tracheostomy and how you can care for it at home.
What is a Tracheostomy?
A tracheostomy is an opening made in your trachea (windpipe) to make breathing easier. A tracheostomy tube is usually put into the stoma (opening) to keep it open.
You may need a tracheostomy if
There is blockage of your airway (e.g. tumour/infection)
You have had surgery in the head and neck area that can cause swelling and blockage of the airway after surgery.
You have difficulty breathing due to neuromuscular or respiratory (lung) conditions, needing frequent clearance of the airway secretions (such as saliva or phlegm) or help in breathing.

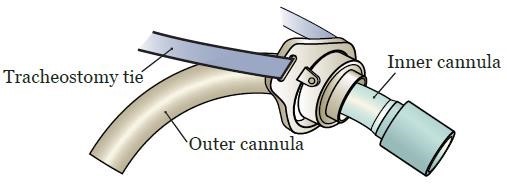
The Tracheostomy Tube
The different parts of a tracheostomy tube are:
Outer cannula The outer cannula fits into the trachea and keeps it open. |  |
| Neck Flange The neck flange is a flat plastic hinge attached to the outer cannula. It has holes on both sides to secure trach ties. These keep the tube from falling out. | |
| Inner Cannula The inner cannula locks into the outer cannula. It should be taken out and cleaned regularly. Cleaning the inner cannula keeps the airway clear of mucus. There are two kinds of inner cannulas:
The colour of the inner cannulas depend on the brand of the tracheostomy. | Shiley inner cannulas Portex inner cannulas  |
| Cuff Some tracheostomies may have a cuff. The cuff is necessary if you need help with • Breathing through a mechanical ventilator/CPAP/BiPAP • Preventing saliva from entering your lungs as much as possible You can tell when a cuff is inflated from an inflated external cuff balloon. Do NOT over inflate the balloon as it can cause pressure injuries to your airway. The medical team will advise you on the appropriate pressure/ volume to inflate. |  |
| Obturator The obturator is used only when the entire tracheostomy tube is changed. It acts as a guide when the outer cannula is put into the trachea. Do NOT leave this in as it will occlude the airflow. This is to be used only with guidance from medical professionals in cases where the tracheostomy tube is dislodged and needs to be reinserted. |  |
| Spigot The spigot is a cap used to cover the tracheostomy when the medical team is preparing to wean you off the tracheostomy. Please only use this with guidance from medical professionals. Do not throw this away. If you have difficulty breathing with the cap on please remove it immediately. |  |
Can I still talk while on tracheostomy?
With the tracheostomy tube in place, airflow is often diverted from your larynx, nose, and mouth. You may not be able to talk the way you do in normal circumstances. Instead, you can communicate through writing or typing.
 The Speech Therapist can help you to talk while on a tracheostomy by using a speaking valve. If you have been given a speaking valve, please
The Speech Therapist can help you to talk while on a tracheostomy by using a speaking valve. If you have been given a speaking valve, please
- Use it for the timing recommended by the Speech Therapist,
- Ensure that the cuff balloon is deflated (if applicable),
- Place it only on the fenestrated inner cannula (with hole),
- Cough phlegm out through the mouth as much as possible,
- Remember to change to the white non-fenestrated inner cannula for suctioning.
It is important to watch out for any signs of difficulty using a speaking valve or when the spigot is in place.
Signs of difficulty include:
- Oxygen saturation level (SpO2) less than 90% (if patient have an oximeter)
- Breathing rate quicker than usual
- Shortness of breath
- Not able to cough out secretions
If you have any signs of difficulty while using the speaking valve, immediately:
Remove speaking valve and cough
Perform suctioning if SPO2 does not improve
Please seek medical attention immediately if you continue to feel breathless or uncomfortable after the episode.
Can I eat while on tracheostomy?
You should be seen by a Speech Therapist before eating or drinking while on tracheostomy. Having a tracheostomy can change the way you swallow, and may cause food or drink to be aspirated (go into the lungs instead of stomach).
If a Speech Therapist has advised for you to eat or drink, please follow their recommendations strictly. This will reduce the risk of aspiration.
General precautions while eating or drinking:
Cuff (if present) should be deflated, and you should be on the fenestrated inner cannula while doing so
Wear your speaking valve (if you have been advised to do so).
Please temporarily stop eating and drinking and contact your Speech Therapist if:You are coughing, choking, or have difficulty breathing while eating or drinking
Food or drink is coming out from your tracheostomy
Cleaning your tracheostomy, stoma, and skin
Clean the skin around your tracheostomy stoma at least once a day, or as often as necessary to keep it clean and dry. If you wear gauze around the stoma, change it whenever it gets dirty or wet. Gauze is not always needed but if you have a lot of secretions, it can prevent skin irritation and keep your clothing dry.
It is advisable to clean your inner cannula at least 3 times a day to prevent any mucus from blocking the tube. This will help you to breathe more easily.
 | Wash your hands thoroughly with soap and water. |
 | Use a cotton wool and cooled boiled water to clean under the flange. |
 | Hold the flange with one hand, and use the other hand to remove the inner cannula (you may need to twist the inner cannula or pull on a ring tab). This is to prevent dislodgement of the tracheostomy tube. Remove the inner cannula by sliding it downwards and outwards * DO NOT remove the entire tracheostomy tube. Only the inner cannula should be removed for cleaning. |
 | Rinse the inner cannula with cooled boiled water. Soft brushes can be used to remove secretions. Soaking with sodium bicarbonate can help remove stubborn phlegm. |
 Dry the inner cannula before putting it back. Slide the inner cannula into position and lock it. | |
Suctioning through the tracheostomy tube
If you have a lot of secretions, your doctors may recommend for you to have a suction machine at home. Most people do not need this.
Ensure that the white non-fenestrated inner cannula is used when suctioning to prevent the suction tube from getting stuck in the tube or going up the wrong way.
Changing the tracheostomy tube holders
Tracheostomy tube holders are neck ties that keep your tracheostomy tube in place. They can be washed and should be changed whenever they get dirty. It is important not to accidentally dislodge the tracheostomy tube when you are changing the ties. Always ensure one hand is keeping the tube in place. Get someone to help if you are not comfortable doing this by yourself.
 | Hold the flange of the tracheostomy tube with one hand. Insert one end of the tube holder through the hole on the neck flange and secure this. |
 | Repeat on the other side. Ensure the Velcro attachment is securely fastened and will not come loose |
 | The ties should be snug (i.e. not too loose or too tight). You should be able to insert just one finger between your neck and the tie comfortably. |
 | Cut off any excess length to the tube holder. |
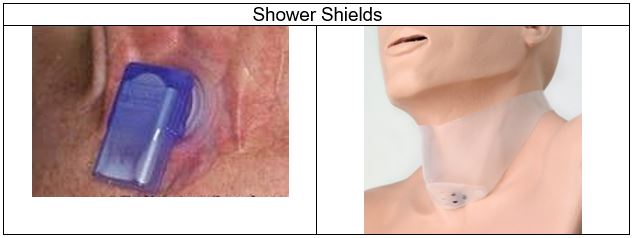
Bathing and Showering with the Tracheostomy
People with a tracheostomy can still shower, but you should be careful to keep water from getting into the tracheostomy tube and stoma. You may prefer to take a bath instead of a shower. If you do take a shower:
- Point shower head to lower chest and stand with your back to the water.
- You can also buy a “shower shield” from the Speech Therapy Department or pharmacy.
- For men, take care to cover your tracheostomy tube when shaving.
Dealing with Emergencies
* Get help and attention immediately
Complete blockage of tracheostomy tube and cannot breathe
- Remove the inner cannula.
- If it is still blocked and suction is available, pass the suction tube down the outer cannula gently to suction out any mucus plug. Do not push with force if you encounter any resistance.
- If the above step fails, remove the whole tracheostomy tube. Only do this in dire situations.
Tracheostomy tube falls out
- Do not panic. If you had the tube for some time it is likely that the stoma will not close off immediately.
- Gently reinsert the tracheostomy tube. Contact your doctor to let them know about the incident.
- If there is difficulty reinserting, do not force the tube in.
Please go to the nearest hospital Emergency Department or call 995 if:
- You are unable to reinsert the outer cannula after accidental removal.
- You are unable to breathe properly after removal of the inner cannula
- Continuous bleeding from the tracheostomy. If you have a tracheostomy tube with a balloon cuff, inflate it while waiting for help.
- Fever of more than 38OC.
If you wish to clarify any of the above information, you can contact your primary doctor through the operator or ward nurse clinician in-charge:
- Operator (Singapore General Hospital) 62223322, to direct call to SDDC Head & Neck Centre (within ENT Centre)
- National Cancer Centre (Office hours only) 64368000, to direct to Head & Neck Nurse.
Contributed by
The information provided is not intended as medical advice. Terms of use. Information provided by SingHealth.
Our Medical Specialists
1
2
3
4
5
Health Articles


Stay Healthy The Easy Way
Get trusted health advice, offers and more.
Stay Ahead in Healthcare Industry
Subscribe to our exclusive updates for healthcare professionals.












Keep Healthy With
Follow SingHealth





© 2026 Singapore Health Services Pte Ltd. All Rights Reserved.