



Let us help you find what you’re looking for.
Popular Searches
What is - Kidney Dialysis
Normal functioning kidneys filter the blood and remove waste and excess salt and water.. Kidney failure is also known as end-stage kidney disease, where the kidney function has declined to the point that it is no longer working. Without renal replacement therapy, kidney failure can lead to death. Renal replacement therapy" is another term for the different treatments for kidney failure, including dialysis and kidney transplantation. Kidney transplantation will be discussed separately.
Dialysis refers to an artificial means of removal of the waste substances from the body using a specialised membrane. There are two types of dialysis: Haemodialysis and peritoneal dialysis.
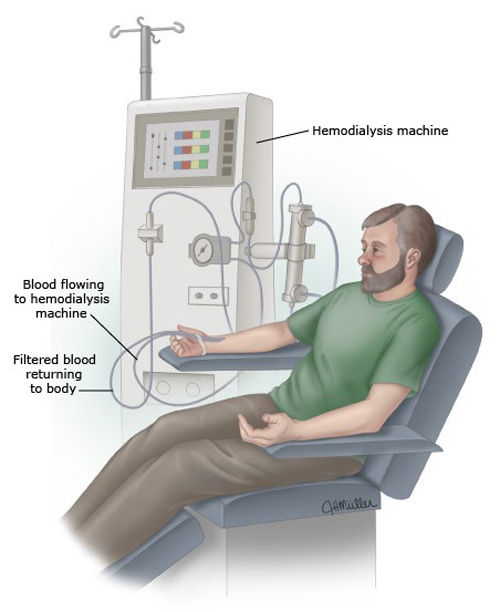
Haemodialysis
Hemodialysis is a procedure in which a dialysis machine takes over the job of the kidneys. In haemodialysis, a mechanised blood pump is needed to draw blood from the patient. The blood is circulated into the machine and passes along a specialised membrane (a dialyser), which essentially functions as an artificial kidney. Waste substances from the blood move across the membrane into a "solution" called dialysate by a physical process called diffusion. The cleaned blood exits the dialyser and is returned back to the patient.
In haemodialysis, the patient needs to have a surgically created vein that is large enough and with a high enough blood flow to allow efficient and adequate dialysis. The surgeon will create this specialised vein called an arterio-venous fistula (aka vascular access) by connecting 2 blood vessels together. Usually, the operation is done initially at the wrist, but other sites along the arm can also be chosen. Sometimes patients' veins are too small for such surgery. Under these circumstances, the surgeon may create vascular access by placing a graft that essentially functions as an artificial blood vessel connecting two adjacent blood vessels. This artificial graft is left permanently under the skin of the patient and is repeatedly cannulated for dialysis.


Peritoneal Dialysis
Peritoneal dialysis is a procedure that people do at home every day. A permanent tube (called a tenchkoff catheter) is placed under sterile conditions into the abdominal cavity in peritoneal dialysis. A specialised fluid called dialysate is filled into the abdomen using this tube. Peritoneal membrane is the membrane lining the abdomen that can function like a dialyser membrane. Waste substances present in the blood flowing through the blood vessels of the abdomen itself move across the peritoneal membrane into the dialysate. The used dialysate with waste products is then drained out of the abdomen via the tenchkoff catheter and discarded. Fresh dialysate is filled back into the abdomen to continue dialysis.

Treatment for Kidney Dialysis
How do I choose between the different treatment options?
Every patient who has kidney failure and facing the prospect of dialysis will usually ask the following questions. "Which is the best form of dialysis?" and "Which one is the most suitable for me?" The answer is not simple. One form of dialysis is not necessarily superior to another. As each patient is different, the treatment they choose must eventually be acceptable to themselves, their families and caregivers. Thus, either treatment may be the best form of treatment for an individual patient. Sometimes, the treatments are chosen because of varying lifestyles, ease of access to a dialysis centre, family support, and medical issues. You, your doctor, and your family will need to work together to find the treatment that's right for you.
PD nevertheless may have certain advantages over HD in certain groups of patients.
- PD benefits patients with heart diseasePD is a slow continuous therapy. The dialysate remains in the abdomen for 4-6 hours before being exchanged with fresh dialysate. During the 4-6 hours, dialysis continues to occur in the patient. The patient is free to continue with his routine work. Even while the patient is asleep, PD dialysate is left in the abdomen overnight. As dialysis is slow and continuous, there is less strain on the heart.
- Dialysis and bleeding tendenciesA group of drugs called anticoagulants are frequently required in long term HD patients. In HD patients, blood is drawn out from the enlarged vein (called an arterio-venous fistula or AVF) into tubing that runs into the dialysis machine. The blood under normal circumstances will thicken (i.e. clot up) into a gel unless the blood is thinned with a type of drug called an anticoagulant. Not all patients, however, tolerate these drugs well. With PD, since no blood drawing is involved, the routine use of these anticoagulants can be avoided. Thus, some patients who have a higher bleeding tendency are better off on PD.
- PD allows more versatile dialysis schedulesPatients on PD can, within limits, adjust their dialysis schedules more easily to fit their daily routines. Unfortunately, haemodialysis patients usually have fixed schedules for dialysis. Whether this is an advantage is something for the individual patient to decide and depends on their lifestyles, workplace and motivation.
- PD avoids blood pressure swingsCertain patients have wide swings in blood pressure as they move from a lying to a standing position. This is called orthostatic hypotension. Wide blood pressure swings make conventional haemodialysis difficult. Patients with this condition would benefit from peritoneal dialysis, which allows for more gentle and gradual fluid removal hence would cause lesser swings in blood pressure.
- PD allows needling to be avoidedSome patients have very small veins, and it is challenging to create a vascular access that would last long enough. PD offers an alternate dialysis modality, which does not require vascular access. The fear of repeated needling for some patients makes PD a more suitable treatment option as it does not require needles.
- The diet allowed on PD is more liberalIrrespective of the modality, dialysis patients must be well-nourished to maximise their benefits on dialysis. PD patients generally require a higher protein and calorie-rich diet than HD patients do. Although the restrictions on phosphate-rich foods are similar to those of HD patients, PD patients have a more liberal choice of potassium-rich food. Patients on PD are generally allowed more fruit which is high in potassium, as they tend to lose more potassium than HD patients.
- PD patients have ease of travellingPD patients benefit from simple home-based therapy, which allows versatility of relatively greater ease of travel when needed. PD patients can also travel with their PD equipment if required. On the other hand, patients on HD need to make special arrangements with overseas dialysis centres to receive their dialysis if travelling overseas. In the absence of dialysis services in certain destinations, HD patients may find travelling more challenging.
- PD patients require less erythropoietin than HD patientsPatients on PD usually require only lower doses of injections (erythropoietin) to build up their blood count levels compared to those on HD. Patients with kidney failure often suffered from anaemia, which means their blood haemoglobin counts are low. This can cause symptoms such as tiredness, feeling cold, lethargic, and in the long term, can worsen heart disease. This problem is usually treated with injections of erythropoietin, which can be once or twice a week. Patients on PD are generally less prone to anaemia than HD patients. They often require fewer erythropoietin injections to boost their blood counts.
- PD patients usually need lesser iron supplements compared to HD patientsIron is a unique mineral that the body needs to make adequate red blood cells. Patients on HD need iron because some of this is lost during the process of haemodialysis. In PD, there is no iron loss from the dialysis. PD patients may still need to take the iron but usually in lesser amounts.Most patients will be able to do well with either form of renal replacement therapy. Each patient is different. Do ask your doctor for their opinions and evaluation before making a final choice.
Healthy Eating While on Dialysis
Dialysis patients need to be careful about their choice of foods. Dialysis cannot replace the kidneys function totally. Because of this, patients will need to continue to be wary about what they eat.
The type of diet recommended differs between haemodialysis and peritoneal dialysis patients. Individual preferences also vary a great deal. It is essential that patients see a dietician discuss a meal plan that is varied and palatable enough to eat well and adequately.
General Principles:
Fluids: It is usually important to restrict fluids to that which matches the fluid output in patients. Excessive fluid intake will accumulate in the body and cause leg-swelling, breathlessness and heart disease.
Salt Restriction: Salt makes a person thirsty and causes one to drink more fluids than they can handle. Salt restriction is a critical feature in dialysis patients' diet plans.
Protein intake: When a patient starts dialysis, they will need a lot of protein every day as part of their meals. Patients who start dialysis are usually undernourished. They may not have eaten well for some time and had repeated hospitalisations and infections that had resulted in lots of weight loss. Hence patients are advised to eat more protein. Protein is usually found in meats like chicken, pork, beef and mutton. Certain foods like soya beans or legumes also contain a lot of protein. However, these particular protein sources are not recommended for dialysis patients. They contain large amounts of phosphate, which a dialysis patient cannot handle well (See paragraph on phosphate).
Carbohydrates: Patients should eat adequate carbohydrates as part of their daily diet to provide them with energy. The protein intake will be consumed for energy generation rather than the desired body muscle mass building with inadequate carbohydrate intake.
Potassium: Patients on haemodialysis, in particular, should restrict their potassium as they undergo dialysis only three times a week. In between dialysis, their potassium levels can rise to dangerous levels if they have high potassium meals. Fruits, in particular bananas, durians, grapes and dried fruit, are very high in potassium. On the other hand, patients on peritoneal dialysis are usually allowed to have a diet higher in potassium because they lose potassium constantly through their form of dialysis.
Phosphate restriction: An average patient on dialysis takes about 1.5gm of phosphate a day, of which 60% or 900mg are absorbed without phosphate binders. Dialysis cannot effectively remove this phosphate from the body. On average, only 300mg of phosphate are removed by PD each day and 700mg by HD over a 4-hour session (which also works out to 300mg per day for a thrice per week haemodialysis schedule). Retained phosphate can accumulate to dangerously high levels and cause renal bone disease and vascular disease complications. Medicines called phosphate binders must be taken to reduce the total amount of phosphate absorbed. Just as important, a patient must restrict himself from foods high in phosphate to reduce the total absorbed phosphate. These include legumes (beans, nuts, lentils, and corns).
Common Medicines a Person on Dialysis Will Need to Take
Dialysis cannot correct all the abnormalities that occur with kidney failure. Most patients will require several medications to treat kidney failure. These medications will be in addition to the other medications they need to take for other non-kidney related diseases. Some of the common medications that dialysis patients need to be on are listed below.
Supplementary vitamins: Dialysis causes a loss of certain substances like water-soluble vitamins and folate from the body. These are easily replaced by taking supplementary vitamins daily, which are usually prescribed as part of medications.
Phosphate binders: This type of medication should be taken with meals. This medication binds to excess phosphate in the meal so that there is no excessive absorption of phosphate. Kidneys that function normally can easily remove excess phosphate that is absorbed after a meal. In kidney failure, patients cannot clear phosphate from the body. Furthermore, dialysis cannot remove phosphate very efficiently either. To prevent an excessive buildup of phosphate, dialysis patients should take phosphate binders with their meals. Phosphate binders should be taken together with meals to maximise their efficacy to bind phosphate. There are different kinds of phosphate binders falling into two broad groups. They are calcium-based binders (calcium carbonate, calcium acetate, calcium hydroxide and calcium citrate) or non-calcium-based binders (lanthanum, sevelamer and velphoro). A dialysis patient may require varying types of phosphate binders in varying amounts, based on their needs, dietary intake, duration on dialysis and tolerance to the medication. These drugs, in general, can cause constipation. Calcium-based phosphate binders may cause high blood calcium levels in certain patients, causing calcium deposition outside the bone when high blood phosphate levels.
Erythropoietin: This is given in injections, usually under the skin, at intervals between 2 and 10 days. This medication brings up the blood stores in the body. A low blood count is a problem for patients with kidneys failure. It causes them to feel cold, tired, lethargic, unable to think, and contributes to worsening heart disease in the long term. Prior to the development of this medication, patients with renal failure required multiple blood transfusions. With erythropoietin injections, patients feel better and need fewer blood transfusions. Like all medications, it is not without side effects. It can cause a worsening of hypertension or flu-like symptoms of chills and body aches, both of which are usually transient.
Iron supplements: Patients on dialysis usually lack a mineral called iron. This contributes to the problem of low blood count. Most dialysis patients require iron supplements, although the requirements may be higher in patients on haemodialysis or those with other reasons for chronic iron losses. There are different preparations, but this medication can generally cause constipation. Laxatives and a high-fibre diet can help to improve constipation.
Antihypertensive medication: This refers to blood pressure medication. Ideally, a patient on dialysis will not need high blood pressure medication. However, a group of patients, whether on peritoneal dialysis or haemodialysis, will continue to require these medicines. There are multiple types of high blood pressure medication with various limitations and efficacy, best discussed with the attending physician. Uncontrolled blood pressure can lead to heart disease and stroke. It is important for kidney failure patients to regularly take their high blood pressure medications to maintain the blood pressure in the normal range.
Complications of Dialysis
All medical treatments potentially have side effects or complications. Dialysis likewise, whether peritoneal or haemodialysis, similarly have potential problems. The problems in dialysis include:
Access complications: For HD patients, the arteriovenous fistula can become blocked and non-functioning, infected, ballooned out (aneurysmal) and rupture. For PD patients, the tenkhoff catheter can be infected at its contact at the skin (exit site infection), or within the tract of the abdomen (tunnel infection), or within the abdomen (peritonitis). It can become blocked or kinked or may leak. Antibiotic therapy cures most cases of infections. These complications can be treated with medicines (e.g. antibiotics for infections) or appropriate surgery in most instances. However, alternate temporary access into a new vein in the neck or chest or groin may need to be inserted with a blood catheter until the original problem is solved.
Heart disease: The heart can be affected in many ways in dialysis patients. The heart's lining can become filled with fluid that compresses the heart (pericarditis), and the heart's blood vessels can become clogged up (atherosclerosis or a heart attack). The valves of the heart can become thickened or infected (bacterial endocarditis). Kidney failure patients also tend to have too much water in their bodies. If uncorrected by a combination of careful fluid and salt restriction and adequate fluid removal by dialysis, fluid overload can lead to overstretching of the heart muscle with permanent damage to the heart (cardiomyopathy)
Vascular Diseases presenting as strokes or gangrene: Patients on dialysis have an increased propensity for strokes (a sudden brain attack with paralysis, numbness or coma) and gangrene (inadequate blood supply causing the death of the organ) of the lower extremities.
Fluid overload: Fluid overload refers to a condition where there is too much salt and water in the body. This manifests as breathlessness or swelling of the legs, hands and abdomen. This can be avoided with adequate dialysis and restriction of fluids.
Malnutrition: The patient on dialysis is prone to malnutrition. Malnutrition is dangerous to the patient. Patients who are malnourished at the start of dialysis have a much higher risk of death than those who are not. The key to preventing malnutrition is to ensure that patients have an adequately high diet in proteins (for a building block) and calories for energy. While a low protein diet is appropriate in the early stage of chronic kidney disease, the converse is true that patients on dialysis should be on a high protein diet. In addition, they should receive adequate dialysis.
Kidney Dialysis - Other Information
Contributed by
The information provided is not intended as medical advice. Terms of use. Information provided by SingHealth.

Our Medical Specialists
Get to know our doctors at SingHealth Hospitals in Singapore.
Get to know our doctors at SingHealth Hospitals in Singapore. here.
Our Medical Specialists
1
2
3
4
5
Health Articles


Stay Healthy The Easy Way
Get trusted health advice, offers and more.
Stay Ahead in Healthcare Industry
Subscribe to our exclusive updates for healthcare professionals.












Keep Healthy With
© 2025 SingHealth Group. All Rights Reserved.